Manejo Cirúrgico de Aneurisma da Artéria Coronária Descendente Anterior com Fístula: Um Raro Relato de Caso do Suriname
Barra lateral de artigos
Conteúdo do artigo principal
Resumo
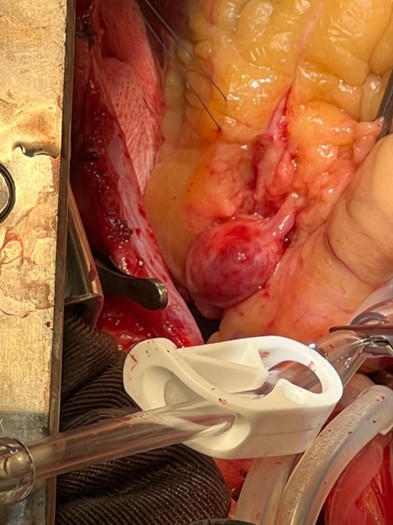
O aneurisma da artéria coronária (AAC) e a fístula da artéria coronária (FAC) são anomalias cardiovasculares raras, e sua ocorrência simultânea é extremamente incomum. Este caso destaca os desafios diagnósticos, terapêuticos e logísticos do manejo de tais anomalias em um cenário de baixos recursos. Apresentamos uma mulher de 56 anos com diabetes, hipertensão e hipotireoidismo que desenvolveu um infarto agudo do miocárdio sem supradesnivelamento do segmento ST (IAMSSST) em maio de 2023, quase dois anos após ser diagnosticada com um aneurisma sacular na artéria descendente anterior (DA) proximal (15,5 × 19,2 mm) com duas conexões fistulosas (31,9 mm e 20 mm). A conduta conservadora inicial foi escolhida devido à estabilidade da paciente e às limitações do centro cirúrgico durante a pandemia de COVID-19. Apesar da terapia medicamentosa otimizada, com aspirina 80 mg/dia, clopidogrel 75 mg/dia, sinvastatina 40 mg/dia e bisoprolol 5 mg/dia, a piora dos sintomas levou à reparação cirúrgica de urgência. O aneurisma e as fístulas foram ligados e foi realizado um enxerto de artéria mamária interna esquerda (AMIE) para a DA. As complicações pós-operatórias incluíram congestão pulmonar e pneumonia, ambas tratadas com sucesso. A paciente permanece assintomática no acompanhamento de dois anos. Em anomalias das artérias coronárias anatomicamente complexas, a intervenção cirúrgica pode oferecer uma opção de tratamento definitivo. Nosso caso enfatiza a importância de estratégias adaptáveis e específicas para cada caso na assistência cardiovascular em ambientes com recursos limitados.
Detalhes do artigo

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Authors retain the copyright of their articles and grant the journal the right of first publication under the Creative Commons Attribution (CC BY) license, which allows others to share and adapt the work with proper attribution.
Referências
Kawsara A, Núñez Gil IJ, Alqahtani F, Moreland J, Rihal CS, Alkhouli M. Management of coronary artery aneurysms. JACC Cardiovasc Interv. 2018;11(13):1211-23. https://doi.org/10.1016/j.jcin.2018.04.003.
Li D, Wu Q, Sun L, Song Y, Wang W, Pan S, et al. Surgical treatment of giant coronary artery aneurysm. J Card Surg. 2017;32(11):767-71. https://doi.org/10.1111/jocs.13172.
Swaye PS, Fisher LD, Litwin P, Vignola PA, Judkins MP, Kemp HG, et al. Aneurysmal coronary artery disease. Curr Cardiol Rev. 2016;12(2):123-30. https://doi.org/10.2174/1573403x12666160516103604.
Latson LA. Coronary artery fistula: How to manage them. Tex Heart Inst J. 2017;44(2):130-2. https://doi.org/10.14503/THIJ-17-6275.
Syed M, Lesch M. Coronary artery fistula: A review. Arch Cardiovasc Dis. 2020;113(1):47-53. https://doi.org/10.1016/j.acvd.2019.09.002.
Güvenç TS, Tutar HE, Şaşmazel A, Erer D. Left anterior descending coronary artery compressed by a giant coronary fistula aneurysm: A case report. Eur Heart J Case Rep. 2019;3(1):ytz002. https://doi.org/10.1093/ehjcr/ytz002.
Kamiya H, Yasuda T, Nagamine H, Shimura T, Kanazawa T, Uchida T, et al. Systematic review of 1007 patients with coronary artery aneurysm and fistula (2002–2021): Outcomes of surgical versus percutaneous treatment. Ann Thorac Surg. 2022;114(3):982-90. https://doi.org/10.1016/j.athoracsur.2022.03.046.